Laparoscopic Gastric Bypass
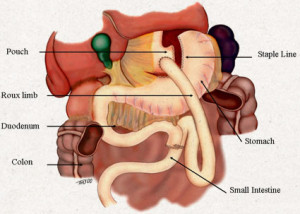 This is one of the two operations supported by the 1991 “NIH Consensus Conference on Surgery for Obesity”. Laparoscopic Roux Y Gastric Bypass has proven, over multiple studies, to achieve significantly greater and more sustained weight loss. It is a combination of two procedures in which a restriction, or a small stomach, is created, as well as a malabsorbtion, through which not all of the small intestine “sees” the food. With this procedure, an average weight loss of excess body weight is 70 – 80% possible.
This is one of the two operations supported by the 1991 “NIH Consensus Conference on Surgery for Obesity”. Laparoscopic Roux Y Gastric Bypass has proven, over multiple studies, to achieve significantly greater and more sustained weight loss. It is a combination of two procedures in which a restriction, or a small stomach, is created, as well as a malabsorbtion, through which not all of the small intestine “sees” the food. With this procedure, an average weight loss of excess body weight is 70 – 80% possible.
The techniques of laparoscopic (minimally invasive) surgery initially became available in 1990 for the removal of gallbladders. This type of surgery has extended to hernia surgery, removal of colon, appendix, and correction of reflux (heartburn).
Laparoscopic Roux Y Gastric Bypass is only available to a select group of patients. In addition to cosmetic advantages (reduced scarring) studies have shown that Lap has decreased hospital stays, pain, hernias, lung problems; and has increased the ability to return to work.
Laparoscopic Vertical Banded Gastroplasty
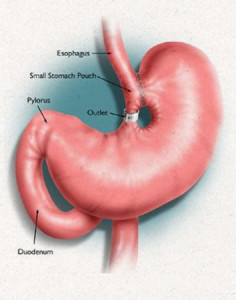 The second procedure approved by the NIH Consensus Panel was Vertical Banded Gastroplasty. It is a simple restrictive procedure in which a small “stomach” pouch is created with a stapler, with the pouch outlet restricted by a silastic band.
The second procedure approved by the NIH Consensus Panel was Vertical Banded Gastroplasty. It is a simple restrictive procedure in which a small “stomach” pouch is created with a stapler, with the pouch outlet restricted by a silastic band.
The disadvantages of this procedure include the technical considerations involved and the fact that weight loss is difficult for “sweet eaters”. Also, the possibility of sustained weight loss is only up to approximately 40 – 50% of excess body weight.
For these reasons, and since a better alternative is available at the same risk, this procedure has not been defined as the “gold standard” by the American Society of Bariatric Surgery.
Laparoscopic Sleeve Gastrectomy
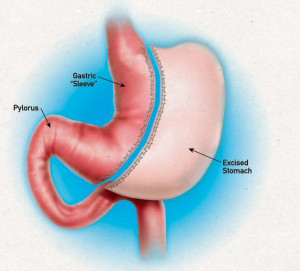 Sleeve gastrectomy is a surgical weight-loss procedure in which the stomach is reduced to about 15% of its original size, by surgical removal of a large portion of the stomach, following the major curve. The open edges are then attached together (often with surgical staples) to form a sleeve or tube with a banana shape.
Sleeve gastrectomy is a surgical weight-loss procedure in which the stomach is reduced to about 15% of its original size, by surgical removal of a large portion of the stomach, following the major curve. The open edges are then attached together (often with surgical staples) to form a sleeve or tube with a banana shape.
The procedure permanently reduces the size of the stomach. The procedure is performed laparoscopically and is not reversible. Initially the sleeve gastrectomy was deemed a first stage of a two stage procedure. Today the ASMBS has recognized the sleeve gastrectomy as a single stage procedure for weight-loss. Since the sleeve became a mainstream procedure in 2004-5, long-term data is not available at this time.
Laparoscopic Adjustable Gastric Banding
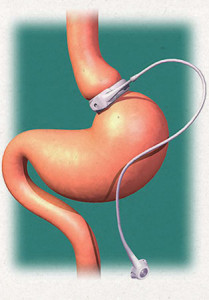 A laparoscopic adjustable gastric band is an inflatable silicone device that is placed around the top portion of the stomach, via laparoscopic surgery, in order to treat obesity. The expandable band is connected to a port placed in the fat of the abdomen and can be adjusted monthly and as needed.
A laparoscopic adjustable gastric band is an inflatable silicone device that is placed around the top portion of the stomach, via laparoscopic surgery, in order to treat obesity. The expandable band is connected to a port placed in the fat of the abdomen and can be adjusted monthly and as needed.
There are currently two types of adjustable bands available in the the United States, Lap-band and Realize band. Placement of the bands are performed via laparoscopy and is quite simple. Patients commitment for success with a band is based on the frequent adjustments, avoiding sweets and incorporating an exercise program.
Revisional Bariatric Surgery
Revisional bariatric surgery is performed to alter or repair a preexisting operation for treatment of morbid obesity. In light of the increasing number of surgical procedures performed, the need to revise/repair operations is also on the rise.
The concept of revisional bariatric surgery is not new. In fact, the first two operations that were widely performed for treatment of morbid obesity were associated with a high rate of revision. The first, jejunoileal (intestinal) bypass, was associated with a large number of severe and unpredictable nutritional problems and diarrhea. Consequently, many of these procedures were revised or reversed.
The second popular operation, stapled gastroplasty (stomach stapling), was associated with many weight loss failures due to both poor design (of the earliest procedures) and the fact that the staples frequently “popped,” thus ruining the operation. The two currently popular procedures, Roux-en-Y gastric bypass and the LapBand, while successful, also require occasional revision. In fact the revision rate for the LapBand is at least 10% during the first two years for either device-related problems or unsatisfactory weight loss. Likewise, the revision rate for gastric bypass is roughly 5-10% over 5 years for either troublesome complications, e.g., ulcer, or unsatisfactory weight loss.